The chest x-ray is the most frequently requested radiologic examination.
In fact every radiologst should be an expert in chest film reading.
The interpretation of a chest film requires the understanding of basic principles.
In this article we will focus on:
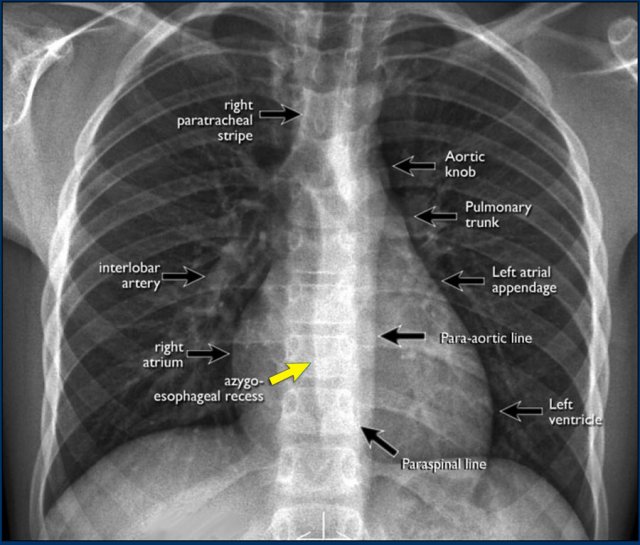
On the PA chest-film it is important to examine all the areas where the lung borders the diaphragm, the heart and other mediastinal structures.
At these borders lung-soft tissue interfaces are seen resulting in a:
These lines and silhouettes are useful localizers of disease, because they can be displaced or obscured with loss of the normal silhouette. This is called the silhouette sign, which we will discuss later.
The paraspinal line may be displaced by a paravertebral abscess, hemorrhage due to a fracture or extravertebral extension of a neoplasm.
Widening of the paratracheal line (> 2-3mm) may be due to lymphadenopathy, pleural thickening, hemorrhage or fluid overload and heart failure.
Displacement of the para-aortic line can be due to elongation of the aorta, aneurysm, dissection and rupture.
The anterior and posterior junction lines are formed where the upper lobes join anteriorly and posteriorly. These are usely not well seen and we will not discuss them.
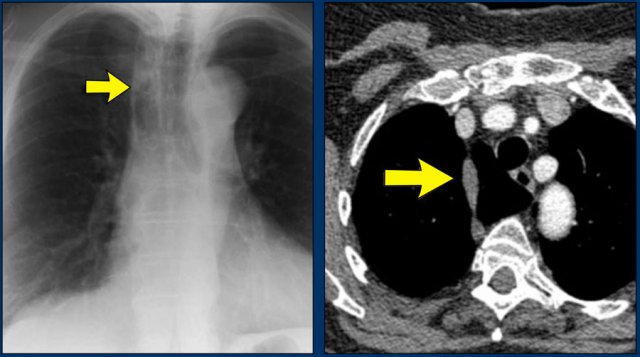
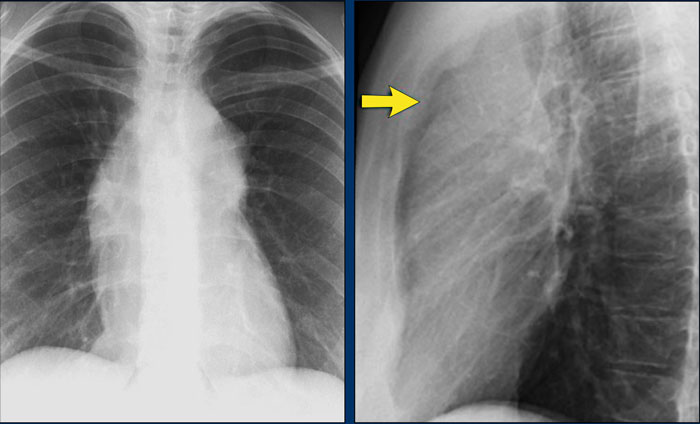
An important mediastinal-lung interface to look for is the azygoesophageal line or recess (arrow).
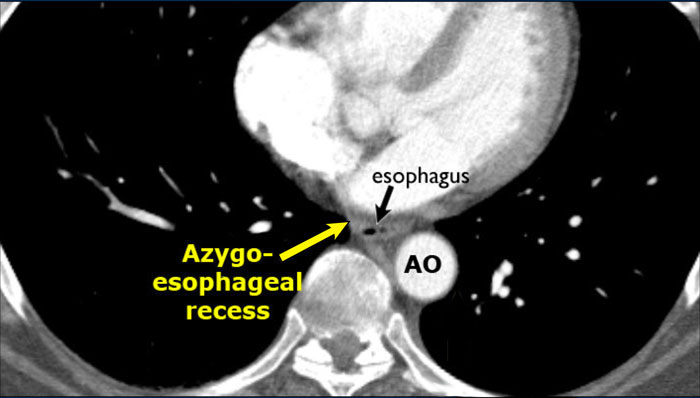
The azygo-esophageal recess is the region inferior to the level of the azygos vein arch in which the right lung forms an interface with the mediastinum between the heart anteriorly and vertebral column posteriorly.
It is bordered on the left side by the esophagus.
Deviation of the azygoesophageal line is caused by:
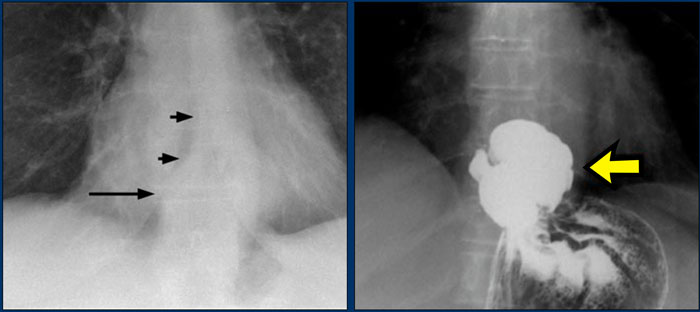
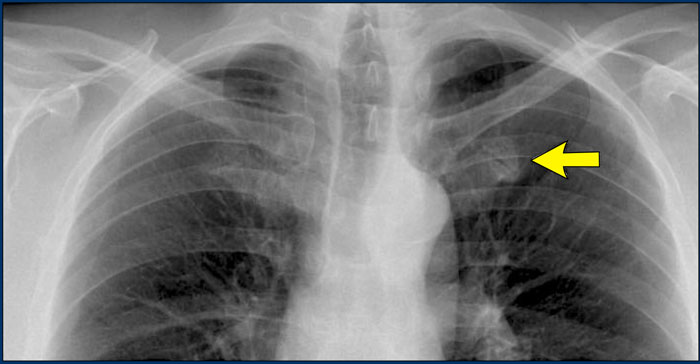
Notice the deviation of the azygoesophageal line on the PA-film.
It is caused by a hiatal hernia.
The arrow point to the barium contrast within the hiatal hernia.
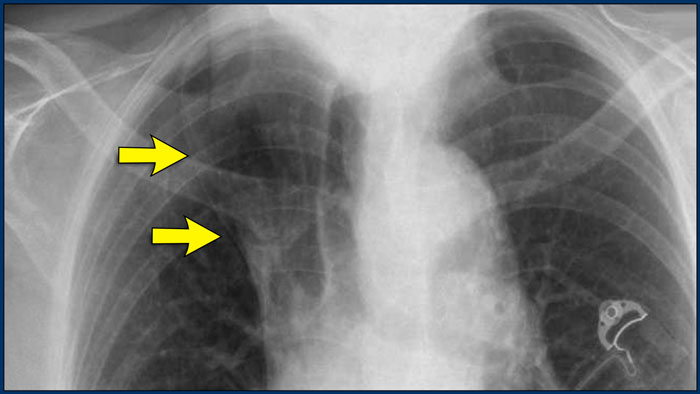
A common normal variant is the azygos lobe.
The azygos lobe is created when a laterally displaced azygos vein makes a deep fissure in the upper part of the lung.
On a chest film it is seen as a fine line that crosses the apex of the right lung.
Here another patient with an azygos lobe.
The azygos vein is seen as a thick structure within the azygos fissure.
In some patients an extra joint is seen in the anterior part of the first rib at the point where the bone meets the calcified cartilageneous part (arrow).
This may simulate a lung mass.
In patients with a pectus excavatum the right heart border can be ill-defined, but this is normal.
It produces a silhouette sign and thus simulating a consolidation or atelectasis of the right middle lobe.
The lateral view is helpful in such cases.
Pectus excavatum is a congenital deformity of the ribs and the sternum producing a concave appearance of the anterior chest wall.
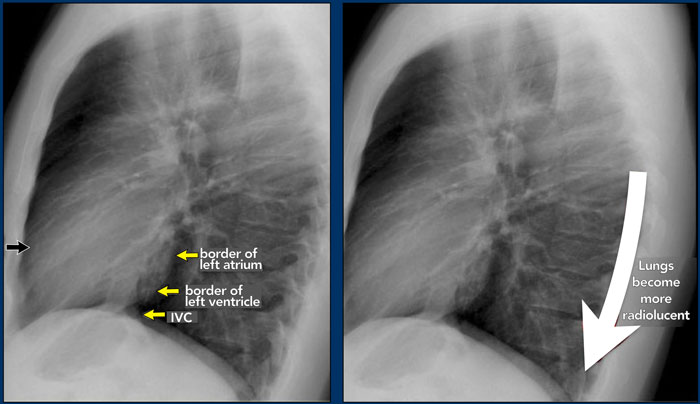
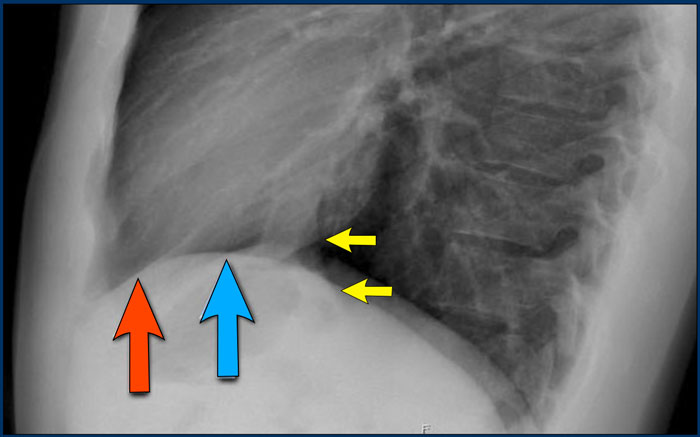
On a normal lateral view the contours of the heart are visible and the IVC is seen entering the right atrium.
The retrosternal space contains air and should be radiolucent down to the level where the right ventricle borders the sternum (small black arrow).
Any radiopacity in this upper retrosternal area is suspective of a process in the anterior mediastinum or upper lobes of the lungs.
As you go from superior to inferior over the vertebral bodies they should get darker, because usually there will be less soft tissue and more radiolucent lung tissue (white arrow).
If this area becomes more dense, look carefully for pathology in the lower lobes.
Diaphragm
The contours of the left and right diaphragm should be visible.
The right diaphragm should be visible all the way to the anterior chest wall (red arrow).
Actually we see the interface between the air in the lungs and the soft tissue structures in the abdomen.
The left diaphragm can only be seen to a point where it borders the heart (blue arrow).
At that point the interface is lost, since the heart has the same density as the structures below the diaphragm.
Pulmonary vessels
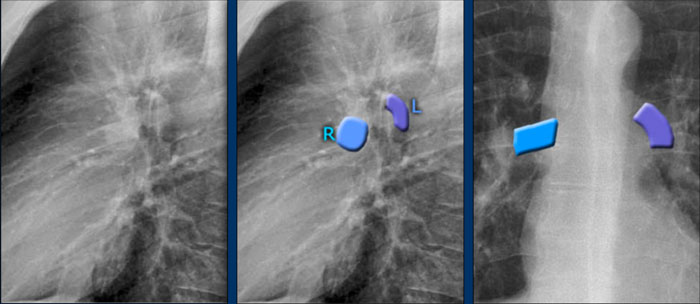
The left main pulmonary artery (in purple) passes over the left main bronchus and is higher than the right pulmonary artery (in blue) which passes in front of the right main bronchus.
Once you know how the normal hilar structures look like on a lateral view, it is easier to detect abnormalities.
In this case on the PA-view there is hilar enlargement.
On the PA-view it is not clear whether this is due to dilated vessels or enlarged lymph nodes.
On the lateral view there are round structures in areas where you don't expect any vessels. So we can conclude that we are dealing with enlarged lymph nodes.
This patient has sarcoidosis.
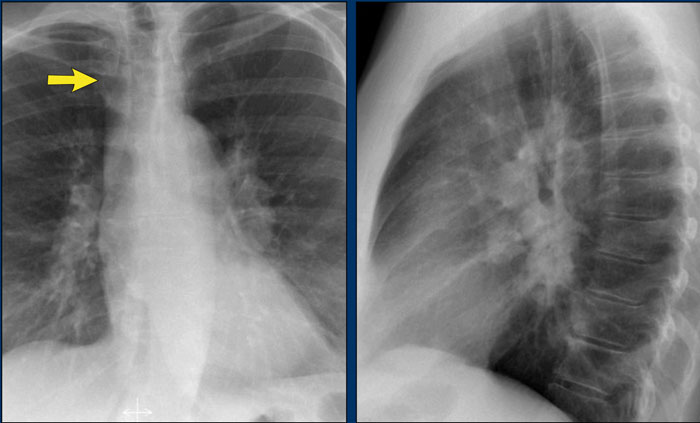
Notice also the widening of the paratracheal line (or stripe) as a result of enlarged lymph nodes.
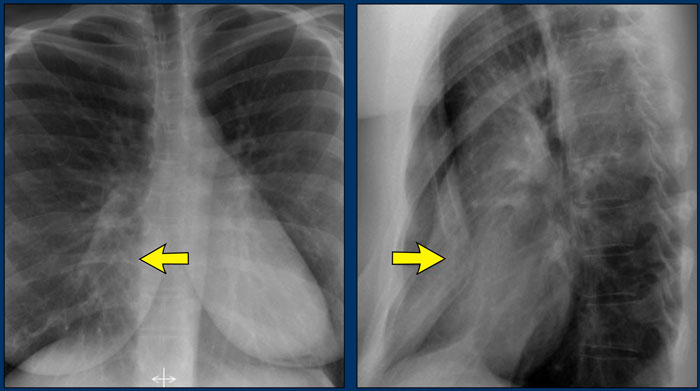
On the lateral view spondylosis may mimick a lung mass.
Any density in the area of the vertebral bodies should lead you to the PA-film to look for spondylosis, which is usually located on the right side (arrows).
On the left side the formation of osteophytes is hampered by the pulsations of the aorta.
On the PA-view the superior mediastinum is widened.
The lateral view is helpful in this case because it demonstrates a density in the upper retrosternal space.
Now the differential diagnosis is limited to a mass in the anterior mediastinum (4 T's).
This was a Hodgkins lymphoma.
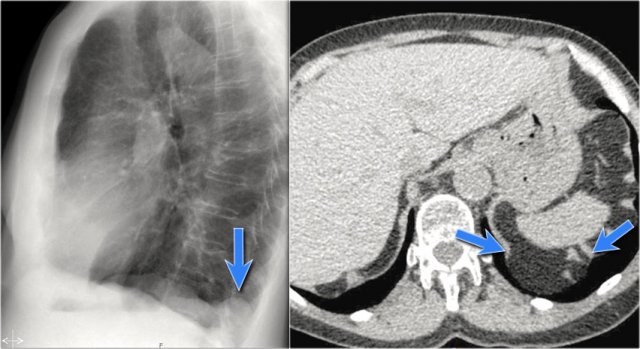
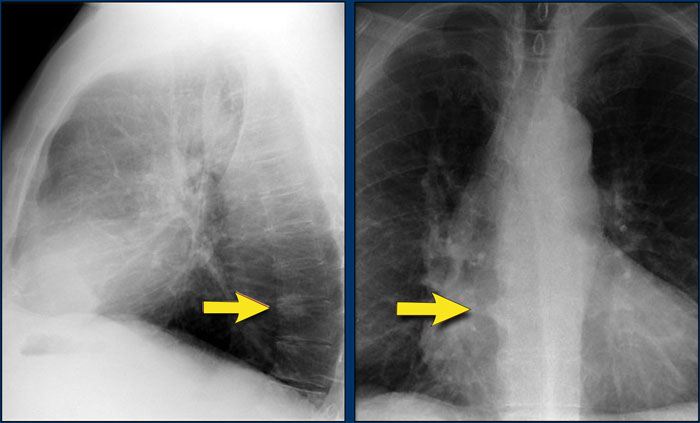
A common incidental finding in adults is a Bochdalek hernia, which is due to a congenital defect in the posterior diaphragm (arrows).
In most cases it only contains retroperitoneal fat and is asymptomatic, but occasionally it may contain abdominal organs.
Large hernias are sometimes seen in neonates and can be complicated by pulmonary hypoplasia.
A hernia of Morgagni is also a congenital diaphragmatic hernia, but is less common.
It is located anteriorly.
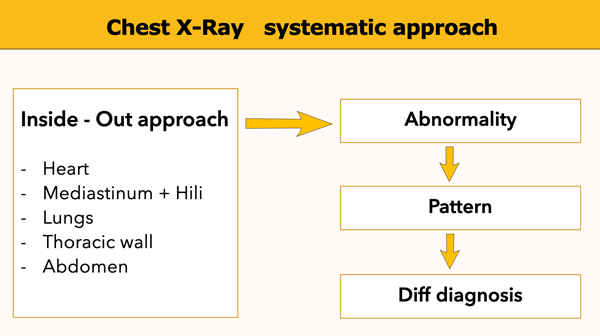
Whenever you review a chest x-ray, always use a systematic approach.
We use an inside-out approach from central to peripheral.
First the heart figure is evaluated, followed by mediastinum and hili.
Subsequently the lungs, lungborders and finally the chest wall and abdomen are examined.
You have to know the normal anatomy and variants.
Find subtle abnormalities by using the sihouette sign and mediastinal lines.
Once you see an abnormality use a pattern approach to come up with the most likely diagnosis and differential diagnosis.
It is extremely important to always compare with old films, as we will demonstrate in this case.
Actually someone said that the most important radiograph is the old film, since it gives you so much information.
For instance a lung mass, which hasn't changed in many years is not a lung cancer.
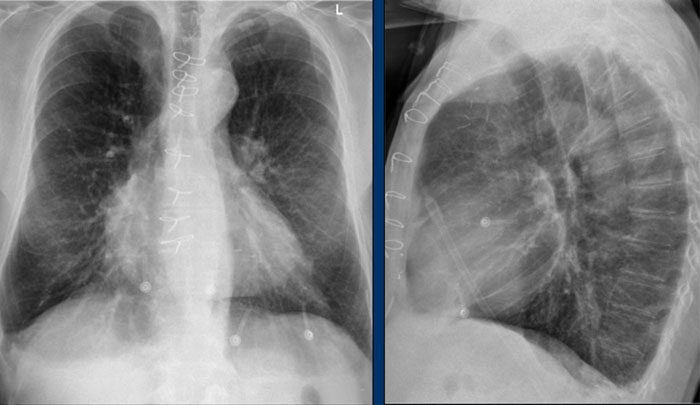
First study the chest films.
Based on these films, you could make the diagnosis of congestive heart failure, but the findings are subtle.
Continue with the old film.